Cheong Wen Xuan

About
With a background in mass communication and client-facing roles, Wen Xuan is a designer who brings strong skills in listening, facilitating dialogue and navigating diverse perspectives. These experiences shape her approach which is grounded in clarity, empathy and connection.
Her practice is built on co-creation rather than designing from a single perspective, allowing her to uncover root causes and surface gaps that often go unnoticed. She believes the most meaningful insights and applicable solutions emerge when designing with people, not just for them.
As a designer driven by curiosity about how things work behind the scenes, she is interested in applying her human-centred design skills across multiple fields to shape more inclusive and thoughtful experiences, and more collaborative ways of creating them—within the systems, services and environments people encounter every day.

The final practical co-design toolkit system uses a visual system of colour-coded zones, numbered task sequences and mapped movement paths that enables participants to translate daily experiences into spatial data. This makes previously unspoken workflows visible, shared and discussable, allowing inefficiencies and patterns to be collectively understood rather than individually absorbed.
Humanising the clinic: To embed empathy into clinical environments, enhancing patient experience while supporting clinical teams
"How do we design clinical environments that improve patient centred-care experiences while responding to the lived realities of those who move through and sustain them every day?"
Humanising the Clinic reveals how both patient experience and clinic workflows are deeply interconnected and continuously shaped through everyday interactions, movement and care. In partnership with the National University Hospital (NUH) Ophthalmology Clinic, this project examines how healthcare spaces can better balance patient experience with staff workflow efficiency.
Ethnographic fieldwork, participatory research sessions and co-design sessions revealed that behind visible operations are improvised decisions, constant communication and continuous small adjustments made by staff, particularly Patient Care Associates (PCAs).
This project focuses on a physical co-design toolkit designed to bridge the gap between non-designers' lived experiences and designers' spatial knowledge, creating a shared language between them. The toolkit is designed to be intuitive and structured so that it is accessible to both non-designers and designers. It uses simple tactile materials and measurement tools to combine the precision of design thinking for designers with accessibility for non-designers, grounding abstract design conversations with spatial representation.
This project sheds light on the invisible labour of PCAs by externalising the physical and cognitive demands of their work, giving form to often overlooked labour. It creates a shared language bridging experience, labour and spatial design, positioning those with an intimate understanding of the system as co-authors in its reconfiguration instead of subjects of a study.
Ultimately, Humanising the Clinic reframes design as participatory, creating tools that enable lived experiences, hidden workflows and overlooked perspectives to become visible, discussable and collaboratively reshaped. It positions healthcare design not as the creation of fixed solutions, but as an ongoing process of collective understanding, adaptation and care, where more empathetic clinical environments are continuously shaped by the people who sustain them and not just for them.

Ethnographic fieldwork was conducted to uncover hidden problems within the clinic through observation and shadowing of patients and clinical staff. Insights were synthesised into a patient journey map that illustrated the interdependencies of patient experience and staff workflows.



Research methodology and theoretical framework
Humanising the Clinic is grounded in ethnographic fieldwork, participatory research and co-design, with the support of NUH Ophthalmology Clinic. Rather than a top-down problem-solving approach, the project focuses on how everyday experiences, workflows and spatial systems are shaped by the people who sustain them.
Through ethnographic fieldwork methods such as shadowing and observation, patient journeys and staff workflows were examined from entry and testing to consultation, payment and medication collection. This helped establish a grounded understanding of the problem before conducting formal in-depth interviews.
The findings were then synthesised into a patient journey map that visually articulated the interdependencies between the patient experience and clinic workflows, surfacing a key insight: dissatisfaction in the patient journey needs to be resolved at a systemic level.
Following the ethnographic fieldwork, a series of participatory research mapping sessions were conducted with doctors, nurses and PCAs to dive deeper into clinical workflows in relation to patient journeys. These sessions were structured while still enabling open-ended conversations with stakeholders.
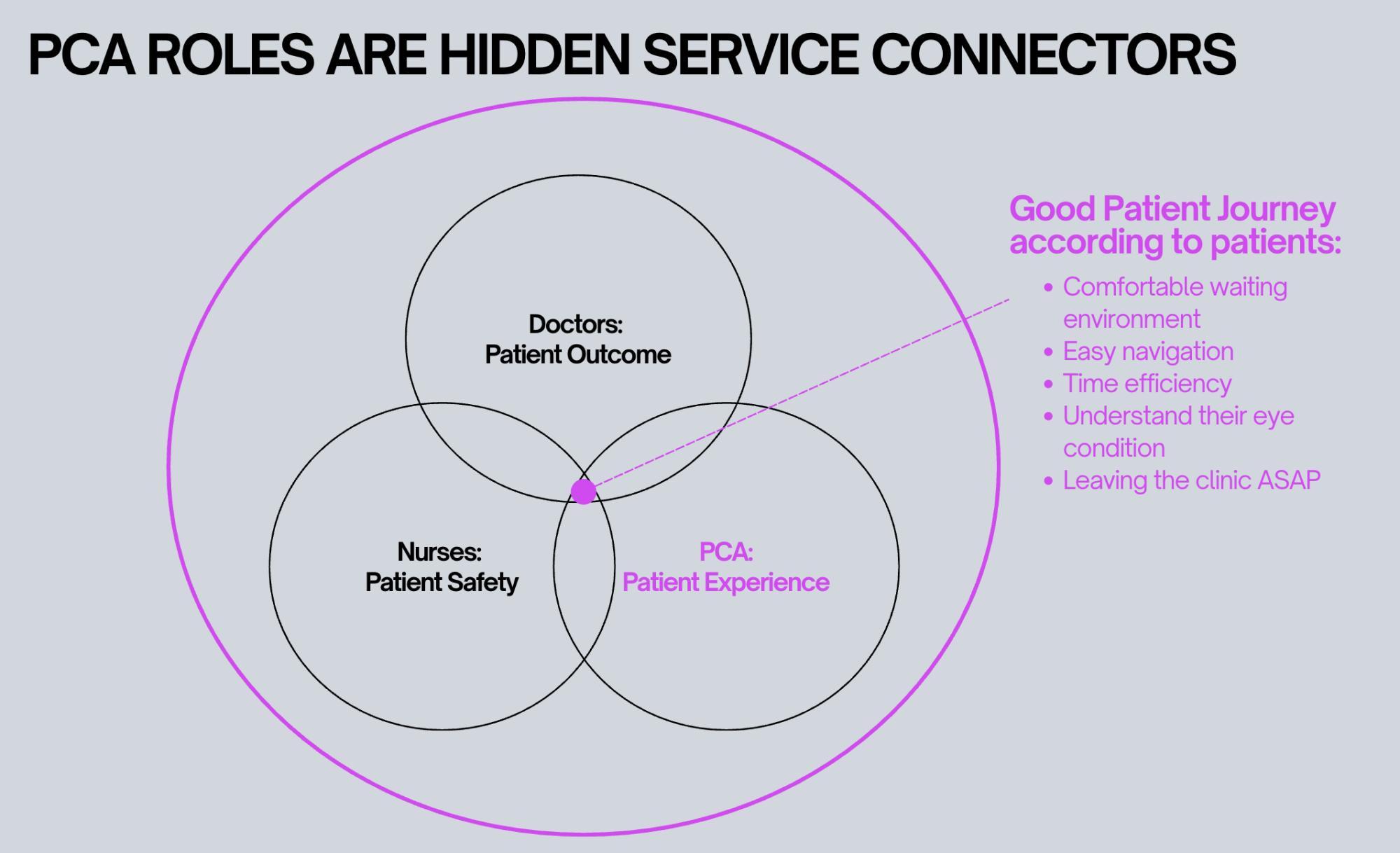
The research uncovered that while all clinic staff work with the patient in mind, their priorities shape how care is carried out—doctors focus on patient outcomes, nurses prioritise patient safety and PCAs focus on the patient journey and movement through the clinic. Understanding these differing perspectives was key to identifying which stakeholders were most closely connected to the lived experience of navigating care.
This led to working closely with PCAs for the remainder of the project, as they emerged as critical yet often overlooked contributors to the patient experience and staff coordinators within the clinic ecosystem.
PCAs, formerly assistants to doctors in consultation rooms, have shifted towards a mobile role within the clinic, supporting patient navigation. Their evolved role positions them between patients, staff and space, as they constantly coordinate movement, manage disruptions and support patients through moments of uncertainty. Despite their intimate understanding of how the clinic functions on the ground, they are rarely included in healthcare design conversations.
Thus, a co-design session was held with PCAs using the co-design toolkit, enabling them to share pain points faced by the patients and within the clinic. Using the insights, PCAs reconfigured the clinic's layout to better suit the needs of the patients, other clinical stakeholders and themselves.
The purpose of these exercises was to understand patient journeys from the perspective of PCAs and empower them to be participate in conversations regarding clinic development. These insights and co-design principles informed the development of the toolkit, ensuring it is intuitive, structured and accessible to non-designers yet grounded enough for it to be understandable to professional designers. The toolkit strategically uses tactile mapping methods, colour-coded systems and spatial visualisation to create a shared language between designers and healthcare staff.
By combining ethnographic fieldwork with participatory co-design methods, Humanising the Clinic reframes design as a collaborative process, one that values lived expertise as essential to shaping more empathetic and patient-centred healthcare environments.
Delia Lee Ru Li

Tan Yee Jing
Syamimi Binti Sabarudin

Nigel Sng Wei Jian

Nur Aliyah Binte Mohammad Noor Azman

Elijah Chia